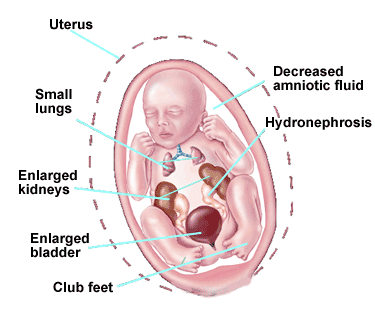
Fetal lower urinary tract obstruction (LUTO) is a rare condition that is caused by a blockage of fetal urination. Because the baby cannot empty the bladder, the baby’s bladder subsequently becomes very large and inflated. Also, because the amniotic fluid is essentially composed of the baby’s urine beyond the middle of the second trimester, the bag of waters dries up. A cascade of secondary effects result in significant morbidity and/or mortality for the baby. This includes problems to the urinary collection system (hydronephrosis) and kidneys (renal dysplasia) attributed to the backpressure from the urinary blockage.
Underdevelopment of the lungs (pulmonary hypoplasia) develops from the lack of amniotic fluid during a critical time of the pregnancy. The cause of fetal LUTO is varied. The most common cause in male fetuses is posterior urethral valves (membrane blocks the flow of urine from the bladder). Oligohydramnios (low amniotic fluid volume defined as the maximum vertical pocket less that or equal to 2.0 centimeters) may then develop, and is associated with a worse prognosis. In females the most common cause is urethral atresia (a body orifice or passage in the body is abnormally closed or absent).
Other causes of fetal LUTO include but are not limited to obstructive ureterocele (area between the tube that carries urine from the kidneys to the bladder), urethral stricture (abnormal narrowing of the urethra) or agenesis (absence of), persistent cloaca (a defect in which the rectum, vagina, and urinary tract are fused together into a single common channel), and megalourethra (congenital dilation of the urethra). The ultrasound findings of many of these conditions are similar, and it is often difficult to differentiate the cause of the urinary obstruction until after delivery. Because there are different causes of LUTO, the prognosis can be expected to be different depending on the individual diagnosis. However, a major component that dictates perinatal outcome is the secondary complications of the obstruction (renal dysplasia and pulmonary hypoplasia). To prevent these complications, several methods have been developed to bypass the blockage of urine while the baby is still in the womb, with the hope that the backpressure on the kidneys can be averted and the amniotic fluid volume may replenish to allow for more normal lung development.
Frequency
Significant lower urinary tract obstruction can be found in 1 in 5000 pregnancies.
Diagnosis and Prognostic Criteria
The diagnosis of LUTO is made by prenatal targeted ultrasound. Typically, the baby’s bladder is very distended (swollen). The presence of a “key-hole” sign is suggestive of posterior urethral valves, particularly in a male fetus. There may be variable degrees of dilation of the upper urinary collection system. The ultrasound findings of the baby’s kidneys should be carefully assessed for evidence of damage. Assessment of amniotic fluid volume as well as the presence of other potential structural abnormalities is sought. Once the diagnosis of LUTO is established, the prognosis for survival is then assessed. The baby’s outcomes have been correlated to the kidney function as assessed prior to treatment. There are two methods to determine the prognosis before surgery. These methods are called fetal vesicocentesis, which samples the baby’s urine, and cordocentesis, which samples the baby’s blood. Genetic studies are also performed.
- Fetal Vesicocentesis: Fetal kidney function may be obtained by performing sampling of the baby’s urine by placing a thin needle into the baby’s bladder and draining the urine. If the results of the first drainage are below the threshold values then fetal therapy may be offered. If the first vesicocentesis shows values above the threshold, a repeat vesicocentesis will be performed in 48 hours.
- Cordocentesis: An alternative to vesicocentesis is to perform a cordocentesis. Under ultrasound guidance, a needle is placed in the umbilical cord. Fetal blood is drawn and sent for a serum Beta-2-microglobulin level. If the serum Beta-2-microglobulin level is less than 5.6 then fetal therapy may be offered.
Management Options and Outcomes
The ability to evaluate kidney function is somewhat imprecise. This probably reflects the different diagnoses responsible for the sonographic findings, which do not have a similar prognosis despite comparable fetal urinary findings or vice versa. Despite this limitation, the follow treatment options are available:
- Expectant Management: This approach entails frequent ultrasound assessment to assess progression during the pregnancy. After delivery, pediatric specialists will evaluate the baby and subsequently offer treatments at that time. The risk of this approach is that further kidney and lung damage may occur during the pregnancy. In the setting of oligohydramnios (low amniotic fluid volume), the expected perinatal mortality rate is 77%. Pregnancies where the obstruction only affects one kidney have a very good prognosis. These pregnancies can be monitored regularly by ultrasound and will likely deliver at full term.
- Vesicoamniotic Shunt: Fetal urinary diversion procedures have been performed since the 1980’s. Essentially, a shunt is placed between the baby’s bladder and the amniotic fluid, thus relieving the blockage. This approach is meant to prevent further kidney and lung damage. The final treatment of the obstruction is performed after the birth of the child. In cases that have been determined to be in the favorable prognostic category (see above), the approximate perinatal survival using this treatment approach is 66%, of which half will have significant kidney damage and may need dialysis or kidney transplant. Risks of shunt placement include dislodgement/blockage/malfunction (25%) thus requiring multiple shunt placements during the pregnancy, urinary ascites (leakage of urine from the bladder into the baby’s abdomen), and fetal death (4%).
- Fetal Cystoscopy and Treatment of LUTO: This approach allows for direct visualization of the baby’s bladder, proximal urethra, and ureteral orifices. This approach, which was developed by Dr. Ruben Quintero, has the theoretic advantage of providing a more precise diagnosis. The ability to establish the correct diagnosis prenatally may improve the counseling capacity. In addition, ablation of posterior urethral valves or other in utero endoscopic treatments of fetal lower urinary tract obstruction may be performed. Whether these theoretical advantages translates into improved perinatal outcomes remains to be proven, which is why this and other centers are conducting studies in this regard. Risks from placing a needle or trocar into the fetal bladder include: infection, bleeding, trauma to the baby such as iatrogenic gastroschisis (hole in the abdominal wall lack the protrusion of the abdominal contents into the amniotic cavity), thermal damage to surrounding structures, or fetal death (4%). The details of the possible diagnostic and treatment approaches are detailed below..
Candidacy for Fetal Treatment
The following criteria generally must be met to offer fetal therapy for LUTO:
- Gestational age: 16 weeks 0 days to 30 weeks 0 days.
- Sonographic evidence of LUTO.
- Fetal renal values below threshold shown in items 5 and 6 listed below.
- Twin gestation may be included.
Details of Procedures
The procedure(s) will be performed under local anesthesia. Fetal anesthesia will be delivered to the fetus with a fine needle under ultrasound guidance prior to entering the fetal bladder. Techniques
- Vesicoamniotic catheter placement: A vesicoamniotic shunt will be placed in all cases over a wire guide. This can be done under ultrasound guidance. Endoscopic documentation of adequate shunt placement may be performed as well. Vesicoamniotic shunting may be necessary several times during the pregnancy due to dislodgement of the shunt or continued urinary outlet obstruction.
- Diagnostic Fetal Cystoscopy: After a 2-3 millimeter skin incision is made, and under ultrasound guidance, an operative fetoscope will be inserted through the mother’s abdomen and uterus into the fetal bladder. The bladder wall, mucosa, trigone, and urethra will be the targets of the endoscopic assessment.
- Operative Cystoscopy: If posterior urethral valves are identified, the valves will be ablated using laser energy through a contact YAG laser fiber. Similarly, an obstructive ureterocele may be incised within the fetal bladder with a contact laser fiber. There may be rare circumstances that fetal urethral patency (unblocked condition) may be assessed with a soft wire guide. If patency is documented, a thin transurethral catheter may be placed over a wire guide. Finally, spontaneous or iatrogenic urinary ascites (diversion of urine from the bladder into the baby’s abdomen) may occur. In these cases, access to the fetal bladder may best be achieved by fetal hydrolaparoscopy. An incision is made over the bladder dome with YAG laser energy, until the inside of the bladder can be seen. If the urethra can be accessed and the posterior urethral valves can be ablated, this is done at this point. Otherwise, surgery is completed by placing a peritoneoamniotic shunt.
Postoperative Care
Before birth, it is recommended that ultrasound assessment occur every week for the first four weeks, then every three to four weeks thereafter. Ultrasound parameters of particular importance include the amount of amniotic fluid volume, measurement of the fetal bladder, assessment of the fetal kidneys and urinary collection system, presence of urinary ascites, and location of the vesicoamniotic shunt. After birth, the child will be evaluated by pediatric specialist and may require further tests and treatments.
Additional Resources
Learn more in the Lower Urinary Tract Obstruction Fetal Care Chat.
TREATMENT CENTERS
Filter List: